De richtlijnen van de ESH van 2023 voor de behandeling van hypertensie bevatten een update over de plaats van bètablokkers bij de behandeling van hypertensie.1
Gerandomiseerde, gecontroleerde studies en meta-analyses2-6 hebben aangetoond dat bètablokkers van de eerste en de tweede generatie zoals propranolol, atenolol en metoprolol het risico op cerebrovasculair accident (CVA), hartfalen en ernstige cardiovasculaire accidenten bij patiënten met hypertensie significant verlagen in vergelijking met de placebo. Voor de preventie van ernstige cardiovasculaire accidenten blijken bètablokkers nagenoeg even effectief te zijn als andere antihypertensiva, maar ze zouden minder goed zijn bij de preventie van CVA's.
Het verschil in preventie van CVA's tussen bètablokkers en andere antihypertensiva is misschien toe te schrijven aan kleine verschillen in de bloeddruk die tijdens de behandeling is verkregen, met inbegrip van de centrale systolische bloeddruk, die bepalend kan zijn bij het optreden van een CVA.
Bètablokkers verhogen het risico op het ontstaan van diabetes bij gepredisponeerde patiënten (hoofdzakelijk patiënten met een metabool syndroom). Hun veiligheidsprofiel is minder goed dan dat van blokkers van het renine-angiotensinesysteem. Het aantal patiënten dat de behandeling in de reële klinische praktijk stopzet, is hoger met bètablokkers.7
In de vorige richtlijnen8-10 waren bètablokkers een van de belangrijkste vijf klassen van antihypertensiva. In het algemene behandelingsalgoritme werden ze echter enkel aanbevolen in geval van een specifieke indicatie, bv. bij patiënten met hartfalen, angina pectoris, myocardinfarct of atriumfibrillatie en jonge vrouwen met hypertensie van vruchtbare leeftijd of met kinderwens.
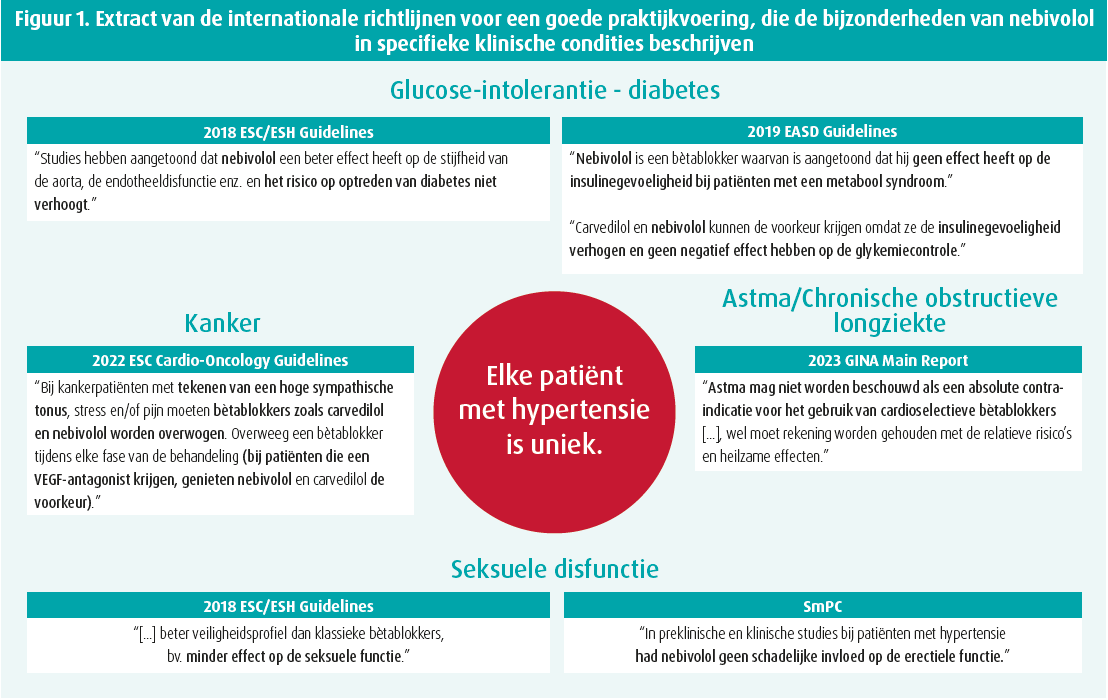
De klasse van de bètablokkers is niet homogeen. Er bestaan enkele farmacologische verschillen tussen de verschillende bètablokkers, waaronder de bèta-1-selectiviteit en directe vaatverwijdende eigenschappen. Bètablokkers van de derde generatie zoals nebivolol en carvedilol hebben een directe vaatverwijdende werking. Volgens studies uitgevoerd met nebivolol en bisoprolol, bèta-1-selectievere bètablokkers, (nebivolol heeft ook een vaatverwijdende werking via afgifte van stikstofmonoxide) hebben die bètablokkers een beter veiligheidsprofiel dan andere en hebben ze onder andere minder bijwerkingen op de seksuele functie.11-12
In de gerandomiseerde, gecontroleerde studies met carvedilol, bisoprolol, metoprolol en nebivolol waren de resultaten beter bij patiënten met hartfalen met een gedaalde ejectiefractie.13 Er zijn echter geen studies uitgevoerd met bisoprolol en vaatverwijdende bètablokkers bij patiënten met hypertensie. In de Verenigde Staten zijn onlangs enkele grote studies met vaatverwijdende bètablokkers gepubliceerd, waarvan de resultaten niet concordant zijn. In een van die studies is geen statistisch significant verschil in cardiovasculaire resultaten vastgesteld tussen nebivolol of carvedilol (n = 118 000) en atenolol (n = bijna 268 000).14 In drie andere studies is een betere cardiovasculaire bescherming vastgesteld met nebivolol dan met atenolol en metroprolol.15-17
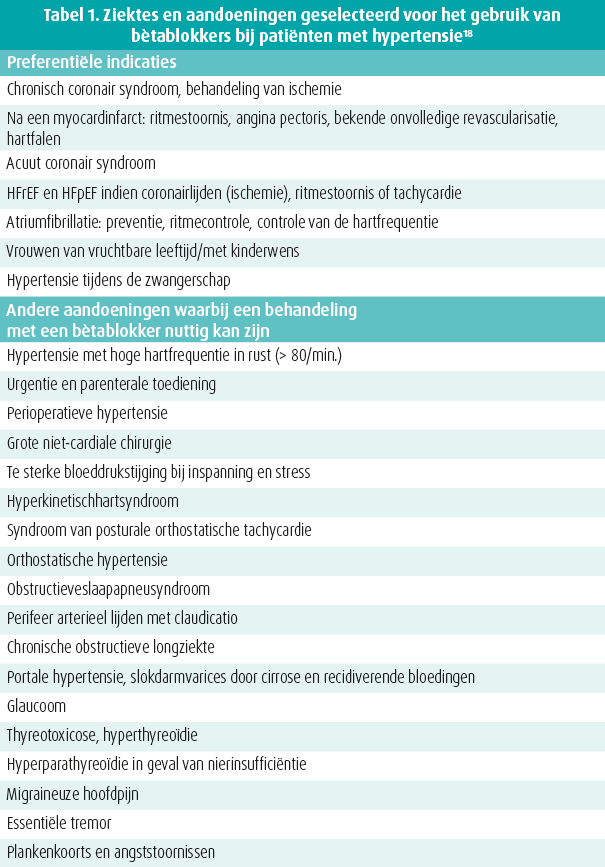
Een recente pragmatische studie heeft het gebruik van bètablokkers bij patiënten met een gegeven ziektebeeld onderzocht (tabel 1).18 Bètablokkers worden blijkbaar overtuigend gebruikt als aanbevolen medische behandeling bij patiënten met een specifieke ziekte, maar hebben gunstige effecten in tal van klinische situaties en met name a) hartziekten al dan niet in samenhang met hypertensie, b) andere bloedvatziekten en c) andere dan cardiovasculaire aandoeningen. Patiënten met hypertensie hebben vaak een hogere hartfrequentie in rust (> 80/min.), wat wijst op een hogere sympathische activiteit.19
Een progressieve stijging van de hartfrequentie in rust gaat gepaard met een progressieve stijging van het risico op atriumfibrillatie, hartfalen en overlijden zowel in de algemene bevolking als bij patiënten met hypertensie.20-22 Het nut van een verlaging van de hartfrequentie bij hypertensie is enkel aangetoond bij post-hocanalyses van gerandomiseerde, gecontroleerde studies23-25, maar volgens de beschikbare gegevens vormen patiënten met hypertensie en een hogere hartfrequentie toch een klinisch fenotype, waarbij bètablokkers geïndiceerd zijn.26
Figuur 1 toont de vele bijzondere eigenschappen van nebivolol.
Tot besluit, de richtlijnen van de ESH van 2023 voor de behandeling van hypertensie herinneren eraan dat bètablokkers geen homogene klasse vormen; integendeel. Bètablokkers zijn niet de eerstelijnstherapie bij een ongecompliceerde hypertensie. De richtlijnen raden bètablokkers wel aan als de hypertensie gepaard gaat met ischemisch hartlijden, een tachyaritmie of hartfalen.
Referenties
- Mancia Chairperson, G., Kreutz Co-Chair, R., Brunström, M. et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J Hypertension, 2023.
- Thomopoulos, C., Parati, G., Zanchetti, A. Effects of blood pressure-lowering on outcome incidence in hypertension: 5. Headto- head comparisons of various classes of antihypertensive drugs - overview and meta-analyses. J Hypertens, 2015, 33 (7), 1321-1341.
- Psaty, B.M., Lumley, T., Furberg, C.D., Schellenbaum, G., Pahor, M., Alderman, M.H., Weiss, N.S. Health outcomes associated with various antihypertensive therapies used as first-line agents: a network meta-analysis. JAMA, 2003, 289 (19), 2534-2544.
- Wei, J., Galaviz, K.I., Kowalski, A.J., Magee, M.J., Haw, J.S., Narayan, K.M.V., Ali, M.K. Comparison of cardiovascular events among users of different classes of antihypertension medications: a systematic review and network meta-analysis. JAMA Netw Open, 2020, 3 (2), e1921618.
- Law, M.R., Morris, J.K., Wald, N.J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ, 2009, 338, b1665.
- Thomopoulos, C., Bazoukis, G., Tsioufis, C., Mancia, G. Beta-blockers in hypertension: overview and meta-analysis of randomized outcome trials. J Hypertens, 2020, 38 (9), 1669-1681.
- Corrao, G., Zambon, A., Parodi, A., Polupatiënteni, E., Baldi, I., Merlino, L. et al. Discontinuation of and changes in drug therapy for hypertension among newly treated patients: a population-based study in Italy. J Hypertens, 2008, 26 (4), 819-824.
- Williams, B., Mancia, G., Spiering, W., Agabiti Rosei, E., Azizi, M., Burnier, M. et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens, 2018, 36 (10), 1953-2041.
- Unger, T., Borghi, C., Charchar, F., Khan, N.A., Poulter, N.R., Prabehandelingakaran, D. et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension, 2020, 75, 1334-1357.
- Whelton, P.K., Carey, R.M. The 2017 Clinical Practice Guideline for High Blood Pressure. JAMA, 2017, 318 (21), 2073-2074.
- do Vale, G.T., Ceron, C.S., Gonzaga, N.A., Simplicio, J.A., Padovan, J.C. Three generations of b-blockers: history, class differences and clinical applicability. Curr Hypertens Rev, 2019, 15 (1), 22-31.
- Viigimaa, M., Vlachopoulos, C., Doumas, M., Wolf, J., Imprialos, K., Terentes-Printzios, D. et al. European Society of Hypertension Working Group on Sexual Dysfunction. Update of the position paper on arterial hypertension and erectile dysfunction. J Hypertens, 2020, 38 (7), 1220-1234.
- Rashid, A.M., Khan, M.S., Fudim, M., DeWald, T.A., DeVore, A., Butler, J. Management of Heart Failure With Reduced Ejection Fraction. Curr Probl Cardiol, 2023, 48 (5), 101596.
- Chan You, S., Krumholz, H.M., Suchard, M.A., Schuemie, M.J., Hripcsak, G., Chen, R. et al. Comprehensive comparative effectiveness and safety of first-line beta-blocker monotherapy in hypertensive patients: a large-scale multicenter observational study. Hypertension, 2021, 77 (5), 1528-1538.
- Egan, B., Basile, J., Punzi, H., Ali, S., Li, Q., Patel, M. et al. Cardiovascular Outcomes with B-blocker Combination Treatment in Patients with Hypertension: a Large, Retrospective Cohort Study. J Am Coll Cardiol, 2018, 71, A1752.
- Huck, D.M., Rosenberg, M.A., Stauffer, B.L. Nebivolol and incident cardiovascular events in hypertensive patients compared with nonvasodilatory beta blockers. J Hypertens, 2022, 40 (5), 1019-1029.
- Basile, J., Egan, B., Punzi, H., Ali, S., Li, Q., Patel, M. et al. Risk of hospitalization for cardiovascular events with b-blockers in hypertensive patients: a retrospective cohort study. Cardiol Ther, 2018, 7 (2), 173-183.
- Mancia, G., Kjeldsen, S.E., Kreutz, R., Pathak, A., Grassi, G., Esler, M. Individualized Beta-Blocker Treatment for High Blood Pressure Dictated by Medical Comorbidities: Indications Beyond the 2018 European Society of Cardiology/European Society of Hypertension Guidelines. Hypertension, 2022, 79 (6), 1153-1166.
- Grassi, G., Quarti-Trevano, F., Seravalle, G., Dell'Oro, R., Facchetti, R., Mancia, G. Association Between the European Society of Cardiology/European Society of Hypertension Heart Rate Thresholds for Cardiovascular Risk and Neuroadrenergic Markers. Hypertension, 2020, 76 (2), 577-582.
- Gillman, M.W., Kannel, W.B., Belanger, A., D'Agostino, R.B. Influence of heart rate on mortality among persons with hypertension: the Framingham Study. Am Heart J, 1993, 125 (4), 1148-1154.
- Benetos, A., Rudnichi, A., Thomas, F., Safar, M., Guize, L. Influence of heart rate on mortality in a French population: role of age, gender, and blood pressure. Hypertension, 1999, 33 (1), 44-52.
- Benetos, A., Thomas, F., Bean, K., Albaladejo, P., Palatini, P., Guize, L. Resting heart rate in older people: a predictor of survival to age 85. J Am Geriatr Soc, 2003, 51 (2), 284-285.
- Bohm, M., Brueckmann, M., Eikelboom, J.W., Ezekowitz, M., Fräßdorf, M., Hijazi, Z. et al. Cardiovascular outcomes, bleeding risk, and achieved blood pressure in patients on long-term anticoagulation with the thrombin antagonist dabigatran or warfarin: data from the RE-LY trial. Eur Heart J, 2020, 41 (30), 2848-2859.
- Julius, S., Palatini, P., Kjeldsen, S.E., Zanchetti, A., Weber, M.A., McInnes, G.T. et al. Usefulness of heart rate to predict cardiac events in treated patients with high-risk systemic hypertension. Am J Cardiol, 2012, 109 (5), 685-692.
- Kolloch, R., Legler, U.F., Champion, A., Cooper-Dehoff, R.M., Handberg, E., Zhou, Q., Pepine, C.J. Impact of resting heart rate on outcomes in hypertensive patients with coronary artery disease: findings from the INternational VErapamil-SR/trandolapril STudy (INVEST). Eur Heart J, 2008, 29 (10), 1327-1334.
- Esler, M., Kjeldsen, S.E., Pathak, A., Grassi, G., Kreutz, R., Mancia, G. Diverse pharmacological properties, trial results, comorbidity prescribing and neural pathophysiology suggest European hypertension guideline downgrading of beta-blockers is not justified. Blood Press, 2022, 31 (1), 210-224.
Niets van de website mag gebruikt worden voor reproductie, aanpassing, verspreiding, verkoop, publicatie of commerciële doeleinden zonder voorafgaande schriftelijke toestemming van de uitgever. Het is ook verboden om deze informatie elektronisch op te slaan of te gebruiken voor onwettige doeleinden.